Iron Deficiency
Created 30 September 2010
Update 20 May 2021 (Included new
case)
Updated 30 January 2026 (Included
new case)
Here’s a
textbook case of iron deficiency. Clearly three years ago the patient was haematologically normal.
|
FIENDISH,GRIMLEY
DOB 13/08/1949 Sex M Pat No
973146 Source
G.P. Address PLANET
EARTH
Clinician CRIPPEN Date 30/09/2010 29/08/2010 13/05/2010 06/11/2008 28/10/2008
12/01/2007 Time u/k
10:25 07:06
u/k
10:03 11:16 Spec AM918276P AW184950Q AW289967S
AM842670E AM830095R AM777490D Test HB
9.0
9.4
11.6
16.2
16.0 16.5 WBC 5.2
5.4
7.9
7.2
5.7 6.3 PLT 413
326
278
194
192 157 RBC 4.68
4.59
4.40
5.15
5.13 5.24 HCT 0.343
0.340 0.380
0.463 0.465 0.481 MCV 73.3
74.1
86.6
89.9
90.6 91.6 MCH 20.9
20.5
26.4
31.5
31.2 31.5 MCHC 28.6
27.6 30.4
35.0
34.4 34.4 NEUH 2.5
2.8
4.4
3.5
2.7 3.6 LYMPH 1.9
1.7
2.4
2.7
2.3 2.1 MONO 0.6
0.7
0.9
0.7
0.6 0.5 EOS 0.1
0.1
0.1
0.1
0.1 0.1 1 View 2 Graph 3 eXit
X
Cursor Down for
more
|
|
|
In the intervening three years the chap has obviously “sprung a
leak” somewhere and his haemoglobin level has
slowly fallen as the platelet count has risen. And as is expected the haemoglobin fell before the red cell volume did (see
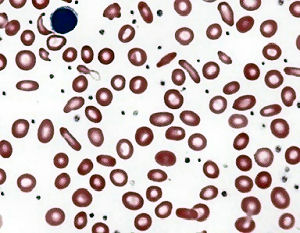
result of 13 May 2010). The blood film shows the characteristic
hypochromia and microcytosis as well as pencil cells. In the first
instance a course of ferrous sulphate would deal with the symptoms, but
clinical investigation to find the leak would be a sensible course of action |
|
And here’s
another case: Look how the haemoglobin level has dropped over eighteen
months. And with that slow and steady drop so the cell volume has dropped
too. |
SPARROW Jack S012345678 21.02.45 F H,21.7127728.A R 03.03.21 Clin. det. -------------------------------------------------------------------------------- HBM WBCM
PLT HCT RBCM
MCVM MCHM MCHCM
RDW N 151118 128
6.32 330 0.413
5.08 81.3 25.2
310 15.3 3.79 270919 113
6.06 349 0.364
4.33 84.1 26.1
310 15.2 3.28 240221 F 45
6.70 654 0.206
3.93 52.4 11.5
218 25.8 4.47 030321 F 50
8.54 365 0.220
3.94 55.8 12.7
227 31.1 6.35 L M
E B RETP
RETA IRF NUC
GF ESR 151118 1.78
0.53 0.16 0.06 2 270919 1.69
0.76 0.27 0.06 10 240221 F 1.27
0.75 0.17 0.04
1.5 60.20 16.2 030321 F 1.25
0.69 0.21 0.04
5.5 223.30 29.9 |
Such reflection isn’t really fooling anyone: I’ve been doing this job
for years. It’s not really news to me at all. But these two cases illustrate
all the features of a chronic blood loss which causes an iron-deficiency anaemia. Characteristically such an insidious onset..
Such so-called “textbook” cases aren’t actually that common. Most
get picked up by the patients presenting much earlier and long before the
changes evident here have set in.
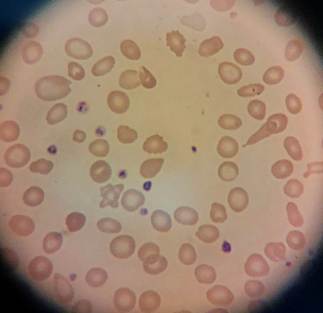
And here’s a young girl with iron
deficiency: (I include this as an example of the camera on my new phone)
|
|
M1234567
OYL Olive 17.07.07 F Specimen H,21.7151009.D
Clin dets Collected 31.03.21 12:24
A.Diag ---------------------------------------------------------------------------- Hb
- 41 |Eosin - 0.01 WBC
- 3.40 |Baso
0.02 Plts
312 |MPV
0.0 Hct
- 0.182 |PCT
0.00 RBC
- 3.28 |NRBC
0.03 MCV
- 55.5 |RETP
3.5 MCH
- 12.5 |RETA + 113.20 MCHC - 225
|IRF 23.5 Neuts
2.02 | Lymphs - 0.99
| Monos
0.36 | DIFF
!Refer to Urgent queue
Microcytosis, hypochromasia and pencil
cells seen |
Here’s a case I saw which made me
think. We can see the MCV and haemoglobin level dropping over a period of eight
years. I’m intrigued by the results at two years in. With the benefit of
hindsight we can see that there’s an iron deficiency slowly getting worse. But
take the results at the two-year stage in isolation. Would anyone *really*
think that anything was amiss?
|
FAKE Name
M1234567
01.01.68 F
--------------------------------------------------------------------------------
HBM WBCM PLT HCT
RBCM MCVM MCHM MCHCM RDW
N 010513
118 6.00 264 0.370 4.29
86.2 27.5 319 13.5 2.76 221015
112 4.90 288 0.361 4.43
81.5 25.3 310 15.2 2.60 210319 F
93 6.01 424 0.323 4.27 75.6
21.8 288 17.9 3.66 190521 F
81 5.90 327 0.290 4.16 69.7
19.5 279 21.1 3.30
L M
E B RETP RETA IRF
NUC GF ESR 010513
2.20 0.45 0.50 0.08
221015
1.70 0.30 0.30 0.10
210319 F
1.48 0.44 0.32 0.11
5 190521 F
1.74 0.55 0.23 0.08
|
And here’s another… wasn’t iron
deficient a year ago
|
|
R,26.3135741.B
R 27.01.26 Clin. det. tired on levetiracetam .
DIFF Blood Film
Review Diagnosis
--------------------------------------------------------------------------------
HBM WBCM PLT HCT
RBCM MCVM MCHM MCHCM RDW
N 251124
118 6.36 261 0.361 3.70
97.6 31.9 327 12.9 3.17 031224
131 8.67 208 0.395 4.08
96.8 32.1 332 12.9 7.61 051224
132 12.61 215 0.404 4.11
98.3 32.1 327 13.0 11.21 270126 F
39 4.92 232 0.160 2.38 67.2
16.4 244 22.4 3.78
L M
E B RETP RETA IRF
NUC GF ESR 251124
2.75 0.36 0.05 0.03
031224
0.72 0.31 0.01 0.02
051224
0.98 0.37 0.02 0.03
270126 F
0.73 0.28 0.11 0.02 1.9 45.20
14.8 ---------------------------------------------------------- |
|
Hypochromic, microcytic with pencil
cells, target cells and tear drop cells. But look at the diagnosis. Levetiracetam
is an anticonvulsant… look it up on-line. Whilst it supposedly doesn’t cause
iron deficiency in and of itself, it is recommended that when on the drug
people should also take iron… |
|

Some More Expert Opinion…